



One in four calls to a healthcare practice books an appointment. That's a 15–25% call-to-appointment conversion rate—one of the highest of any service industry.
And yet most of the agencies running PPC for these practices are bidding the exact same amount on the campaign that drives those bookings as they are on the one that drives "do you take my insurance?" calls.
If agencies deprioritized the campaigns generating low-quality calls and doubled down on the campaigns driving real customers, they would find their conversion rates are actually even higher—and wasted spend would plummet at the same time.
This article breaks down why optimizing on call volume alone is bleeding PPC budget—and how tracking call outcomes by campaign, keyword, and landing page reveals which traffic sources are actually filling your schedule.
Note: Not a WhatConverts user yet? Start your free 14-day trial today or book a demo with a product expert to see how we help prove and grow your ROI.
Google Ads Can't Tell a New Patient from a "Do You Take My Insurance?" Call
Here's the core problem: every call looks identical inside Google Ads.
A caller ready to book a new patient exam and a caller asking about your parking situation both register as conversions. You paid $50+ per click for both. The algorithm treats them as equally valuable signals and optimizes accordingly.
WebFX data shows healthcare CPCs running $3.50–$6.00 for specialized services—climbing higher in competitive urban markets. At those prices, the difference between a 25% conversion rate and a 5% conversion rate isn't a rounding error. It's the difference between a campaign that fills your schedule and one that fills your voicemail.
The problem isn't your campaigns. It's that you have no way to see which campaigns are generating which type of calls.
When You Optimize for Call Volume, You're Flying Blind
Consider a practice running three Google Ads campaigns:
| Keyword | Calls | CPL | Google Ads Verdict | |
| Campaign A | "Family Doctor Near Me" | 90 | $210 | ✓ Strong performer |
| Campaign B | "New Patient Exam" | 40 | $380 | ✗ Cut it |
| Campaign C | "Back Pain Specialist" | 15 | $620 | ✗✗ Way over budget |
Every benchmark metric says double down on Campaign A, and cut B and C.
But when you tag calls by outcome—booked appointment, existing patient, wrong number, insurance inquiry—the picture reverses:
| Calls | Booked Appointments | Conversion Rate | |
| Campaign A | 90 | 5 | 5.5% |
| Campaign B | 40 | 10 | 25% |
| Campaign C | 15 | 4 | 27% |
Campaign A is generating volume. Campaigns B and C are generating patients.
Without outcome data attached to each call, you're optimizing for the wrong number entirely. CPL isn't a performance metric when it's divorced from call quality.
The Calls That Inflate Your "Conversions" Column
The calls dragging down your true conversion rate tend to fall into predictable categories:
- Existing patients: calling to reschedule, request records, or ask about test results. Not new patient revenue.
- Insurance verifiers: calling before they ever commit to booking. High volume, low conversion.
- Wrong-number and spam calls: counted as conversions in Google Ads, completely worthless in your pipeline.
- General inquirers: asking about services broadly with no clear intent to book.
None of these call types is inherently bad. But they're categorically different from a high-intent new patient call.
When they're all counted equally, the keyword that drives insurance inquiries and the keywords that drive booked physicals look identical in your reports.
So your budget keeps flowing to both, and you pay just as much for zero-revenue calls from existing patients as you do for calls from brand new high-value customers.
The Fix: Tag Every Call with What Actually Happened
The solution isn't more calls. It's knowing what's inside the calls you're already getting.
When each inbound call is tagged with its outcome—booked appointment, existing patient, not qualified, wrong number, follow-up needed—a much clearer picture emerges: which campaigns actually drive appointments and which drive cheap junk.
That data does three things:
1. It tells you where to scale.
The campaign converting at 25% deserves more budget, even if its CPL looks "expensive" on paper.
A $380 CPL on a 25%-converting campaign is dramatically more efficient than a $210 CPL on a 5.5%-converting one.
2. It cleans up your optimization signals.
Google's Smart Bidding learns from what you mark as a conversion. If every call counts, the algorithm chases call volume. If only booked appointments count, it starts finding more patients.
3. It reveals keyword-level truth.
"New patient exam" may convert at 30%. "Family doctor hours" may convert at 3%. Both drive clicks, but only one drives revenue.
Where WhatConverts Fits In
Tracking this manually is nearly impossible with standard PPC reporting. That’s where call tracking software comes in.
WhatConverts tracks every inbound call back to the campaign, keyword, and landing page that drove it—then lets you tag each call with its outcome. Booked, existing patient, not qualified, no-show: every call is properly categorized.
Once calls are tagged, your reporting immediately shows:
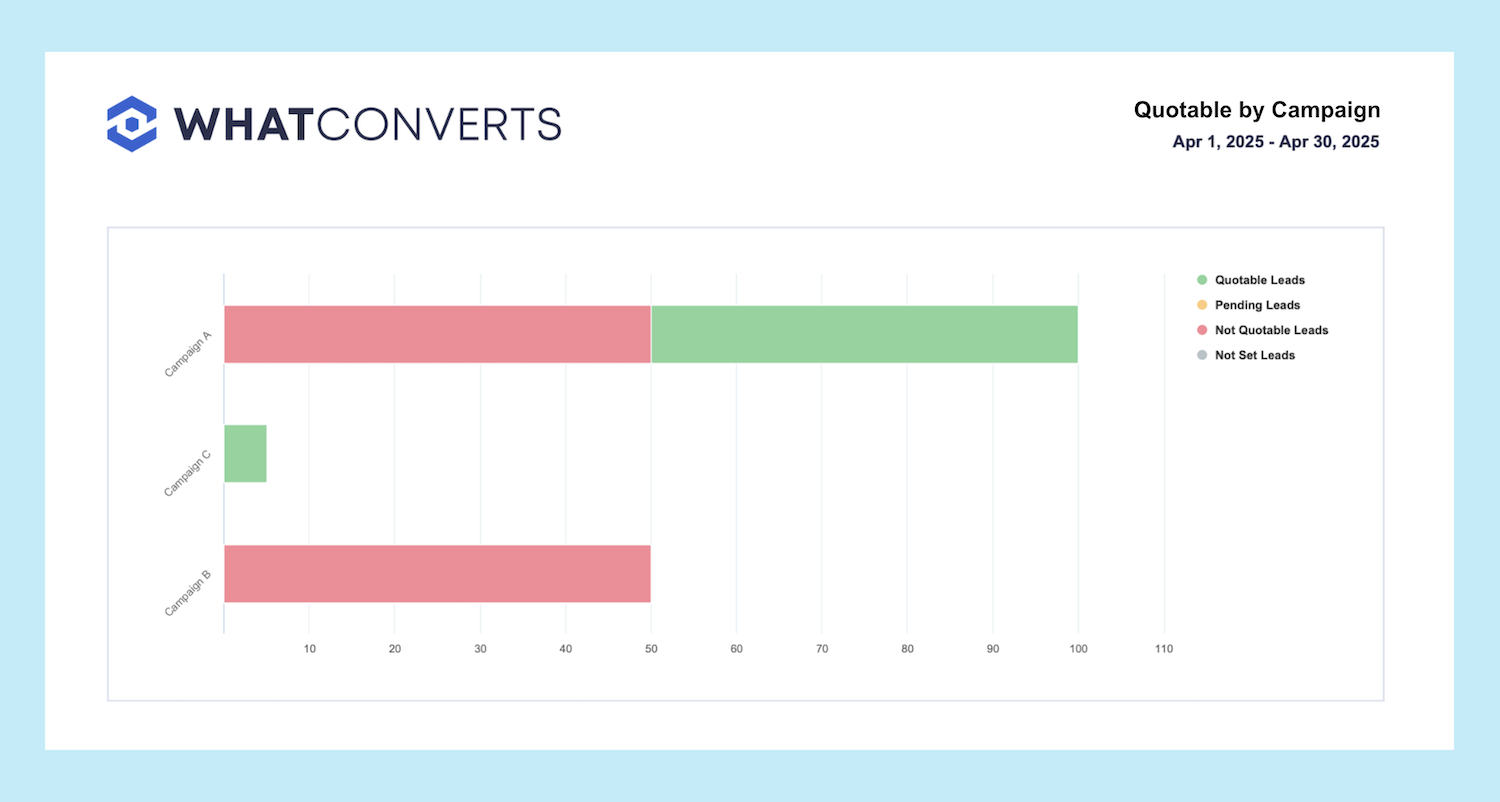
- Which campaigns produce 25% appointment conversion rates
- Which campaigns produce 5% conversion rates
- Which keywords consistently drive booked patients versus insurance inquiries
And because WhatConverts integrates directly with Google Ads, those outcome tags feed back into Smart Bidding as conversion values—teaching the algorithm to find more of the calls that actually book.
The result: your best campaign gets the budget signal it deserves. The junk gets cut.
Proof: What Happens When Campaigns Are Optimized for Qualified Calls
A UK healthcare marketing agency called Klatch ran into the same issue many clinics face: marketing reports showed plenty of “leads,” but the clinics weren’t seeing the same results in their appointment books.
The problem was attribution. Google Ads counted every call as a lead, even though many were low-intent inquiries.
After implementing WhatConverts, Klatch was able to identify which calls were actually qualified patient inquiries and send only those conversions back to Google Ads. That changed how the campaigns optimized.
Within three months, the clinic saw:
- 167% more qualified patient leads
- 30% higher conversion rates
- Campaigns automatically prioritizing searches that generated real patient conversations
The biggest shift wasn’t more traffic—it was better optimization signals.
Read More: Compounding Growth Engine Earns +167% Qualified PPC Leads [Case Study]
The Benchmark That Actually Matters
Healthcare's 15–25% call-to-appointment rate is a compelling industry average. But averages hide the spread.
Your highest-performing campaign may already be converting at 30%+. Your worst may be at 4%. Both are inside that 15–25% average.
The practices that scale PPC efficiently aren't the ones with the lowest CPL. They're the ones who know which calls book and reallocate accordingly.
That clarity starts with tracking what actually happens on the other end of the phone.
Ready to see which campaigns are filling your schedule—and which are just filling your call log?
Start your free 14-day trial of WhatConverts today or book a demo with a product expert to see how we help prove and grow your ROI.
Get a FREE presentation of WhatConverts
One of our marketing experts will give you a full presentation of how WhatConverts can help you grow your business.
Schedule a Demo
Grow your business with WhatConverts




